Download
1 / 27
290 likes | 667 Views
Renin-Angiotensin System. Afferent. Macula Densa. JG Apparatus. Efferent. Factors Affecting Renin Release. Increased By Decreased By. Na + , water retention BP Activation of AT 1 receptors (short loop negative feed back). Arterial BP BP in Glomerular Vessels Loss of Na + , water

E N D
Afferent Macula Densa JGApparatus Efferent
Factors Affecting Renin Release Increased ByDecreased By • Na+, water retention • BP • Activation of AT1 receptors (short loop negative feed back) • Arterial BP • BP in Glomerular Vessels • Loss of Na+, water • Sympathetic activity Renin Release
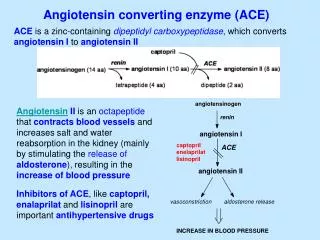
Renin- synthesized, stored and released by exocytosis into renal artery circulation by JG cells • Both renin and prorenin are stored in the JG cells • Prorenin is converted to renin by proteolytic enzymes- proconvertase I or cathepsin B • Concentration of prorenin is about 10 times higher than renin in circulating blood • Renin converts angiotensinogen to angiotensin I which is then converted to angiotensin II by Angiotensin Converting Enzyme (ACE) • Angiotensin II is the active form of the enzyme
Control of Renin Secretion • Macula densa pathway • Intrarenal baroreceptor pathway • -receptor pathway
Macula densa pathway • Specialized columnar epithelial cells in thick ascending limb of the nephron • Lies between the afferent and efferent arterioles adjacent to the JG apparatus • Reabsorption of NaCl occurs by macula densa cells • Changes in NaCl reabsorption modify renin release from the JG cells • Increase in NaCl flux causes inhibition of renin release while decrease causes increased renin release • ATP, adenosine & PG modulate this pathway
Macula densa- control of renin release AngII ATP Na+ 2Cl- K+ Na+-K+-2Cl- symporter + Na+ -ve Feed back K+ AT1 NE release 1 ADP P2Y — Tubular End (Gq-PLC-IP3 - Ca2+ Adenosine PG nNOS A1 (-) (+) Renin Release Adenosine Receptor NO COX-2 PG Macula densa JG Cell
In macula densa, regulation is mainly by concentration of Cl- concentration rather than Na+ concentration • Concentration of Na+ in tubular lumen is usually higher than required for saturating the symporter due to which changes in levels of Na+ do not have much effect on macula densa • Cl- concentrations required for saturation of the symporter are high due to which changes in its concentration mainly effect macula densa mediated renin release
Renin release control: mechanism II- intrarenal baroreceptor pathway • in BP or renal perfusion pressure in preglomerular vessels inhibits renin release and vice versa • May be mediated by stretch receptors in arterial walls or/and by PG synthesis • Mechanism III: via 1 receptors on JG cells
Increased renin secretion enhances formation of angiotensin II which is responsible for short loop negative feed back • Other factors in negative feed back: • Activating high pressure baroreceptors and thereby reducing renal sympathetic tone- k/a long loop negative feed back • Increasing pressure in the preglomerular vessels • Reducing NaCl reabsorption from the proximal tubule (pressure natriuresis) thereby reducing delivery of NaCl to macula densa which reduces renin release
Physiological factors modifying renin release: • Systemic blood pressure • Dietary salt intake • Pharmacological agents- • NSAIDs- inhibit PG synthesis renin release • Loop diuretics decrease BP and increase NaCl reabsorption causing increased renin release • ACE inhibitors, ARBs, renin inhibitors • Centrally acting sympatholytic agents and -blockers decrease renin secretion by reducing -receptor activation
ACE • It is a glycoprotein • It is nonspecific enzyme that catalyzes diverse amino acids • It is identical to Kinase II that inactivates bradykinin and other potent vasodilator peptides • ACE is present in the vascular endothelium which is responsible for rapid conversion of Ang I to Ang II • ACE2: present in human body- carboxypeptidase • It cleaves one amino acid residue from Ang I to convert it to Ang (1-9) and Ang II to Ang (1-7) • Ang (1-7) binds to Mas receptors and elicits vasodilator and non-proliferative responses
ACE2 has 400 fold greater affinity for AngII than AngI • ACE2 is not inhibited by standard ACE inhibitors used • It has no effect on bradykinin • Physiological significance uncertain • May act a a counter-regulatory mechanism to oppose effects of ACE • It regulates effects of Ang II by converting it to Ang (2-8) also called Ang III • Ang IV (3-8) is formed from Ang III • Ang I has is less than 1% potent than Ang II
Angiotensinogen is formed in the liver • Major site for conversion of Ang I to Ang II is the lung • Reason: because it has a large number of capillaries and ACE is present in the endothelial cells of the capillaries • Other sites: other blood vessels specially of kidney • Angiotensinages are diverse group of enzymes like aminopeptidases, endopeptidases, carboxypeptidases and other peptidases that degrade and inactivate angiotensin • They are non-specific enzymes
Local (Tissue) Renin-Angiotensin System • Important for its role in hypertrophy, inflammation, remodelling and apoptosis • Binding of renin or pro-renin to pro-renin receptors located on cell surface • Present in many tissues like brain, pituitary blood vessels, heart, kidney, adrenal glands • Extrinsic local RAS: in vascular endothelium of these tissues • Intrinsic local RAS: tissues having mRNA expression
Number of enzymes that act as alternative pathway for conversion of angiotensinogen to AngI or directly to AngII • Enzymes are: cathepsin, tonin, cathepsin G, chymostatin sensitiveAngII generating enzyme and heart chymase • Angiotensin receptors:two types- • AT1 and AT2 • Most effects of AngII are mediated by AT1 receptors • Role of AT22 receptors not well defined • May counterbalance many effects of AT1 activation
Functions of RAS • Effects of AngII on CVS include: • Rapid pressor respone- peripheral resistance • Slow pressor response- via decrease in renal excretion and production of endothelin-1 • Vascular and cardiac hypertrophy and remodeling
Rapid pressor response: • AT1 receptors are located in the vascular smooth muscle cells • Ang II activates these receptors and constricts the precapillary arterioles and to a lesser extent the postcapillary venules • It stimulates the Gq-PLC-IP3-Ca2+ pathway • Vasoconstriction is maximum in kidneys, lesser in splanchnic. • Weak vasoconstrictor action in brain, lung and skeletal muscles
Other contributing factors are: • Enhancement of peripheral NE neurotransmission by: • Inhibiting reuptake of NE into nerve terminals • Enhancing vascular response to NE • High concentrations of Ang II stimulate ganglion cells directly • CNS Effects: • Increase in central sympathetic outflow • Attenuation of baroreceptor mediated reductions in sympathetic discharge from brain
Brain contains all components of RAS • Brain is affected by both circulating AngII and AngII formed within the brain • Action of AngII on brain causes: • Increased central sympathetic tone • Dipsogenic effect (thirst) • Release of catecholamines from adrenal medulla: AngII depolarises the chromaffin cells of adrenal medulla and causes release of adrenaline
Slow Pressor Response: • Produced by effect on the kidneys • AngII: • Reduces urinary excretion of Na+ and water • Increases excretion of K+ • Stimulates Na+/H+ exchange in proximal tubule due to which Na+, Cl- and bicarbonate reabsorption increases • Increases expression of Na+-glucose symporter in proximal tubule • Directly stimulates Na+-K+-2Cl- symporter in thick ascending limb
Proximal tubule secretes angiotensinogen and the connecting tubule secretes renin • Paracrine tubular RAS? Functions? • AngII stimulates zona glomerulosa of adrenal cortex to increase the synthesis and secretion of aldosterone • Also auguments its response to other stimuli like ACTH, K+ • Aldosterone acts on distal and collecting tubules to cause retention of Na+ and excretion of K+ and H+ • Stimulatory effect of AngII on aldosterone secretion depends on plasma concentrations of Na+ and K+
Release of aldosterone is enhanced in cases of hyponatremia or hyperkalemia and vice versa • Effect on glomerular filtrate: • Constriction of afferent arterioles reduces intraglomerular pressor and tends to reduce GFR • Contraction of mesangial cells decreases the capillary surface area within the glomerulous and tends to decrease GFR • Constriction of efferent arterioles increases the intraglomerular pressor and tends to increase GFR • Normally, GFR is slightly reduced by AngII
Vascular and cardiac hypertrophy and remodeling: • Cells involved- vascular smooth muscle cells, cardiac myocytes and fibroblasts • Stimulates migration, proliferation and hypertrophy of vascular smooth muscle cells • Increases extracellular matrix production by vascular smooth muscle cells • Causes hypertrophy of cardiac myocytes • Increases extracellular matrix production by cardiac fibroblasts
Effect on heart: • Increases cardiac contractility directly by opening of voltage gated Ca2+ channels in cardiac myocyte • Increases cardiac rate indirectly by increasing central sympathetic tone • Increases adrenal release of catecholamines • Facilitates adrenergic neurotransmission • Rapid rise in BP causes baroreceptor stimulation- decrease in central sympathetic tone and increased vagal tone • Net effect-uncertain
Inhibitors of RAS • ACE inhibitors (ACEIs) • Angiotensin receptor blockers (ARBs) • Direct renin inhibitors (DRIs)