Download
1 / 1
10 likes | 81 Views
Magnetic Resonance Imaging (MRI) of the Brain of Infants with Bacterial Meningitis. Carlos Oliveira, MD, Michael Morriss, MD, John Mistrot, Joseph Cantey, MD, and Pablo J Sánchez, MD 3 rd year Pediatric Resident at

E N D
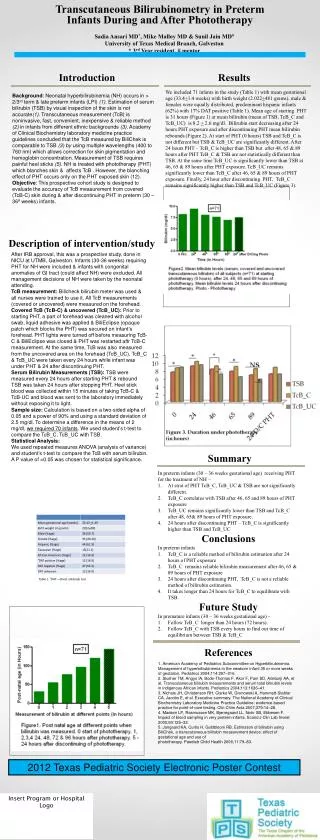
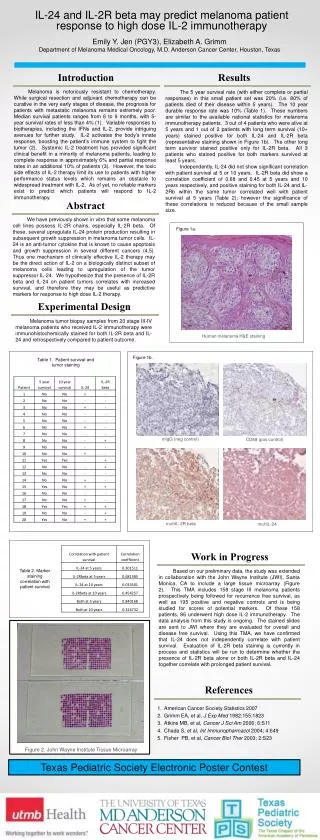
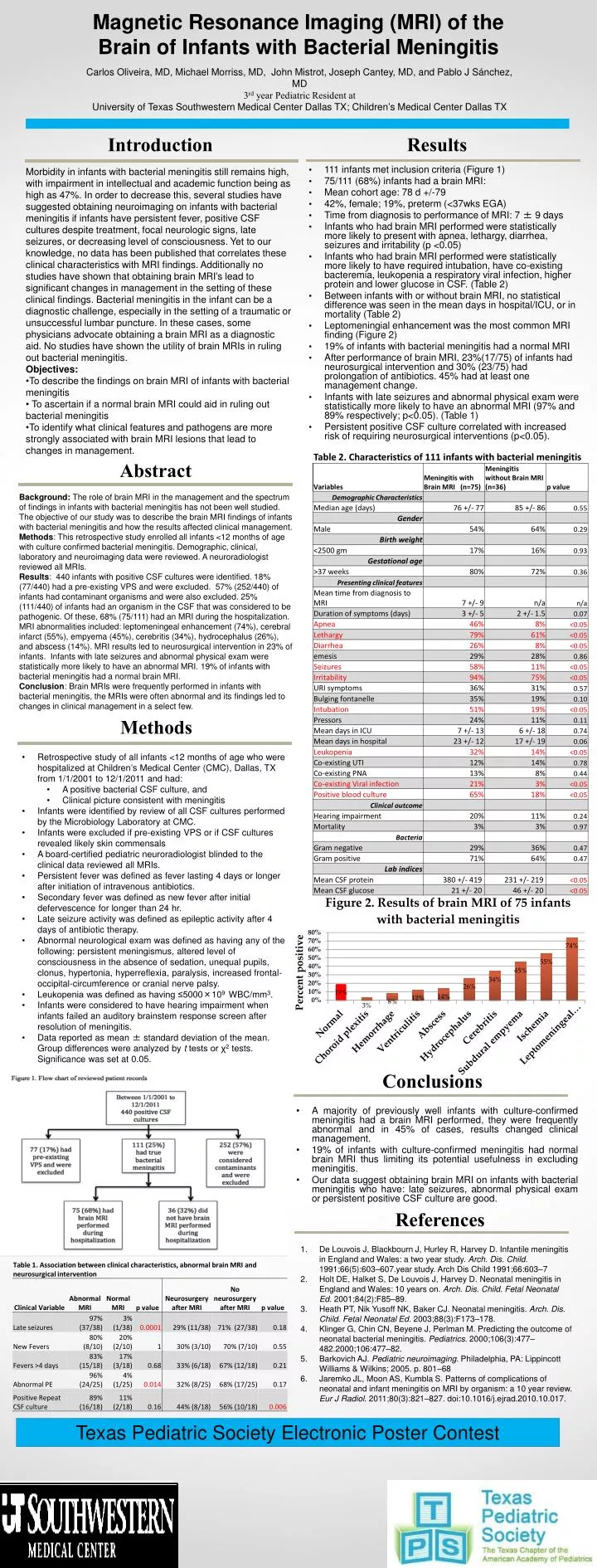
Magnetic Resonance Imaging (MRI) of the Brain of Infants with Bacterial Meningitis Carlos Oliveira, MD, Michael Morriss, MD, John Mistrot, Joseph Cantey, MD, and Pablo J Sánchez, MD 3rd year Pediatric Resident at University of Texas Southwestern Medical Center Dallas TX; Children’s Medical Center Dallas TX Introduction Results • Morbidity in infants with bacterial meningitis still remains high, with impairment in intellectual and academic function being as high as 47%. In order to decrease this, several studies have suggested obtaining neuroimaging on infants with bacterial meningitis if infants have persistent fever, positive CSF cultures despite treatment, focal neurologic signs, late seizures, or decreasing level of consciousness. Yet to our knowledge, no data has been published that correlates these clinical characteristics with MRI findings. Additionally no studies have shown that obtaining brain MRI’s lead to significant changes in management in the setting of these clinical findings. Bacterial meningitis in the infant can be a diagnostic challenge, especially in the setting of a traumatic or unsuccessful lumbar puncture. In these cases, some physicians advocate obtaining a brain MRI as a diagnostic aid. No studies have shown the utility of brain MRIs in ruling out bacterial meningitis. • Objectives: • To describe the findings on brain MRI of infants with bacterial meningitis • To ascertain if a normal brain MRI could aid in ruling out bacterial meningitis • To identify what clinical features and pathogens are more strongly associated with brain MRI lesions that lead to changes in management. • 111 infants met inclusion criteria (Figure 1) • 75/111 (68%) infants had a brain MRI: • Mean cohort age: 78 d +/-79 • 42%, female; 19%, preterm (<37wks EGA) • Time from diagnosis to performance of MRI: 7 ± 9 days • Infants who had brain MRI performed were statistically more likely to present with apnea, lethargy, diarrhea, seizures and irritability (p <0.05) • Infants who had brain MRI performed were statistically more likely to have required intubation, have co-existing bacteremia, leukopenia a respiratory viral infection, higher protein and lower glucose in CSF. (Table 2) • Between infants with or without brain MRI, no statistical difference was seen in the mean days in hospital/ICU, or in mortality (Table 2) • Leptomeningial enhancement was the most common MRI finding (Figure 2) • 19% of infants with bacterial meningitis had a normal MRI • After performance of brain MRI, 23%(17/75) of infants had neurosurgical intervention and 30% (23/75) had prolongation of antibiotics. 45% had at least one management change. • Infants with late seizures and abnormal physical exam were statistically more likely to have an abnormal MRI (97% and 89% respectively; p<0.05). (Table 1) • Persistent positive CSF culture correlated with increased risk of requiring neurosurgical interventions (p<0.05). Abstract Background: The role of brain MRI in the management and the spectrum of findings in infants with bacterial meningitis has not been well studied. The objective of our study was to describe the brain MRI findings of infants with bacterial meningitis and how the results affected clinical management. Methods: This retrospective study enrolled all infants <12 months of age with culture confirmed bacterial meningitis. Demographic, clinical, laboratory and neuroimaging data were reviewed. A neuroradiologist reviewed all MRIs. Results: 440 infants with positive CSF cultures were identified. 18% (77/440) had a pre-existing VPS and were excluded. 57% (252/440) of infants had contaminant organisms and were also excluded. 25% (111/440) of infants had an organism in the CSF that was considered to be pathogenic. Of these, 68% (75/111) had an MRI during the hospitalization. MRI abnormalities included: leptomeningeal enhancement (74%), cerebral infarct (55%), empyema (45%), cerebritis (34%), hydrocephalus (26%), and abscess (14%). MRI results led to neurosurgical intervention in 23% of infants. Infants with late seizures and abnormal physical exam were statistically more likely to have an abnormal MRI. 19% of infants with bacterial meningitis had a normal brain MRI. Conclusion: Brain MRIs were frequently performed in infants with bacterial meningitis, the MRIs were often abnormal and its findings led to changes in clinical management in a select few. Methods • Retrospective study of all infants <12 months of age who were hospitalized at Children’s Medical Center (CMC), Dallas, TX from 1/1/2001 to 12/1/2011 and had: • A positive bacterial CSF culture, and • Clinical picture consistent with meningitis • Infants were identified by review of all CSF cultures performed by the Microbiology Laboratory at CMC. • Infants were excluded if pre-existing VPS or if CSF cultures revealed likely skin commensals • A board-certified pediatric neuroradiologist blinded to the clinical data reviewed all MRIs. • Persistent fever was defined as fever lasting 4 days or longer after initiation of intravenous antibiotics. • Secondary fever was defined as new fever after initial defervescence for longer than 24 hr. • Late seizure activity was defined as epileptic activity after 4 days of antibiotic therapy. • Abnormal neurological exam was defined as having any of the following: persistent meningismus, altered level of consciousness in the absence of sedation, unequal pupils, clonus, hypertonia, hyperreflexia, paralysis, increased frontal-occipital-circumference or cranial nerve palsy. • Leukopenia was defined as having ≤5000×109 WBC/mm3. • Infants were considered to have hearing impairment when infants failed an auditory brainstem response screen after resolution of meningitis. • Data reported as mean ± standard deviation of the mean. Group differences were analyzed by t tests or χ2 tests. Significance was set at 0.05. Conclusions • A majority of previously well infants with culture-confirmed meningitis had a brain MRI performed, they were frequently abnormal and in 45% of cases, results changed clinical management. • 19% of infants with culture-confirmed meningitis had normal brain MRI thus limiting its potential usefulness in excluding meningitis. • Our data suggest obtaining brain MRI on infants with bacterial meningitis who have: late seizures, abnormal physical exam or persistent positive CSF culture are good. References De Louvois J, Blackbourn J, Hurley R, Harvey D. Infantile meningitis in England and Wales: a two year study. Arch. Dis. Child. 1991;66(5):603–607.year study. Arch Dis Child 1991;66:603–7 Holt DE, Halket S, De Louvois J, Harvey D. Neonatal meningitis in England and Wales: 10 years on. Arch. Dis. Child. Fetal Neonatal Ed. 2001;84(2):F85–89. Heath PT, Nik Yusoff NK, Baker CJ. Neonatal meningitis. Arch. Dis. Child. Fetal Neonatal Ed. 2003;88(3):F173–178. Klinger G, Chin CN, Beyene J, Perlman M. Predicting the outcome of neonatal bacterial meningitis. Pediatrics. 2000;106(3):477–482.2000;106:477–82. Barkovich AJ. Pediatric neuroimaging. Philadelphia, PA: Lippincott Williams & Wilkins; 2005. p. 801–68 Jaremko JL, Moon AS, Kumbla S. Patterns of complications of neonatal and infant meningitis on MRI by organism: a 10 year review. Eur J Radiol. 2011;80(3):821–827. doi:10.1016/j.ejrad.2010.10.017. Texas Pediatric Society Electronic Poster Contest Insert Program or Hospital Logo

![[Insert Hospital Name]](https://cdn0.slideserve.com/59021/insert-hospital-name-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/1968686/slide1-dt.jpg)

![[Insert Client Logo]](https://cdn1.slideserve.com/2208608/slide1-dt.jpg)