Download
1 / 32
430 likes | 2.01k Views
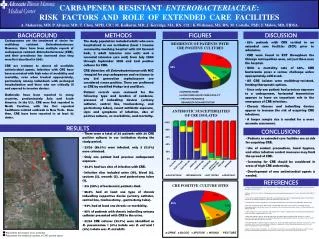
Carbapenem -Resistant Enterobacteriaceae ( CRE) . Wendy Bamberg, MD HAI Medical Epidemiologist Colorado Department of Public Health and Environment. Enterobacteriaceae. Normal human gut flora & environmental organisms Human infections Healthcare-associated infections

E N D
Carbapenem-Resistant Enterobacteriaceae (CRE) Wendy Bamberg, MD HAI Medical Epidemiologist Colorado Department of Public Health and Environment
Enterobacteriaceae • Normal human gut flora & environmental organisms • Human infections • Healthcare-associated infections • Foodborne infections • Community infections (e.g. UTI) • Some of the most common organisms encountered in clinical laboratories • Alishewanella • Alterococcus • Aquamonas • Aranicola • Arsenophonus • Azotivirga • Blochmannia • Brenneria • Buchnera • Budvicia • Buttiauxella • Cedecea • Citrobacter • Cronobacter • Dickeya • Edwardsiella • Enterobacter • Erwinia • Escherichia, e.g. Escherichia coli • Ewingella • Grimontella • Hafnia • Klebsiella • Kluyvera • Leclercia • Leminorella • Moellerella • Morganella • Obesumbacterium • Pantoea • Pectobacterium • CandidatusPhlomobacter • Photorhabdus, • Plesiomonas, • Pragia • Proteus • Providencia • Rahnella • Raoultella • Salmonella • Samsonia • Serratia • Shigella • Sodalis • Tatumella • Trabulsiella • Wigglesworthia • Xenorhabdus • Yersinia, e.g. Yersiniapestis • Yokenella
EnterobacteriaceaeDevelopment of Resistance • Resistance to β-lactams (penicillin, cephalosporins) has been a concern for decades • β-lactamases • Extended-spectrum β-lactamases (ESBLs) • use of carbapenems • Carbapenems – last really good defense against Gram negatives • Resistance to carbapenems developing • Carbapenem-resistant Enterobacteriaceae(CRE) • Only treatment options polymyxins (colistin), and tigecycline
Carbapenem-Resistant Enterobacteriaceae(CRE) • Carbapenemase production • KPC – most common in U.S. • NDM-1 – few cases in U.S., most received medical care in India and Pakistan (one of many metallo-beta-lactamases) • Cephalosporinase + porin loss • Some cephalosporinases have a low level of carbapenem resistance (AMP-C or some ESBLs [CTX-M]) • Porins allow antibiotics into the periplasmic space
KPC-producing CRE in the United States DC HI PR AK Patel, Rasheed, Kitchel. 2009. Clin Micro News CDC, unpublished data Slide courtesy of A. Kallen, CDC Nov, 2006
KPC-producing CRE in the United States DC HI PR AK Patel, Rasheed, Kitchel. 2009. Clin Micro News CDC, unpublished data Slide courtesy of A. Kallen, CDC
Los Angeles County June 2010 – Carbapenem-resistant K. pneumoniae made a reportable condition Over 6 months, 164 cases were detected More prevalent than expected 77 (46%) from long-term acute care (LTAC) hospitals 62 (38%) from skilled nursing facilities One NDM-1 isolate was detected One outbreak was detected in LTAC due to surveillance Confusion among laboratorians between carbapenemase and ESBL-mediated resistance
KPC outbreak, Chicago 2008 Clin Infect Dis 2011;53:532-40.
Prevalence of KPC in a LTCFOhio, 2004 50 patients enrolled • 24 patients excluded: • 16 due to inadequate longitudinal sampling • 8 due to exposure to acute care 26 patients Stool collected for median 11.5 weeks (range 10-26 weeks) 12 (46%) with KPC-producing K. pneumo 8 had KPC for median 9 weeks (range 4-26 weeks) 4 had KPC in only 1 specimen 130 patient facility caring for children and young adults with severe neurodevelopmental conditions Clin Infect Dis 2012;54(9):1314-21.
NDM-1 in the New Delhi Environment From Sept 26 to Oct 10, 2010 Collected swabs of seepage water and public tap water from sites within 12 km radius of New Delhi Samples analyzed for NDM-1 by PCR Samples analyzed for bacterial growth and presence of NDM-1 bacteria Assessed plasmid transfer and temperature Lancet Infect Dis2011;11:355-62.
NDM-1 in the New Delhi Environment Seepage water (n=171) • 51 (30%) positive NDM-1 gene • 171 (100%) grew bacteria on cefotaxime • 166 (97%) grew bacteria on meropenem • 12 (7%) grew bacteria positive for NDM-1 gene Public tap water (n=50) • 2 (4%) positive NDM-1 gene • 50 (100%) grew bacteria on cefotaxime • 14 (28%) grew bacteria on meropenem • 2 (4%) grew bacteria positive for NDM-1 gene Lancet Infect Dis2011;11:355-62.
NDM-1 in India:Species detected Bacteria carrying NDM-1 not previously described Lancet Infect Dis2011;11:355-62.
NDM-1 in India:Species detected Bacteria causing gastroenteritis Lancet Infect Dis2011;11:355-62.
Mean temperatures in New Delhi and Ideal Plasmid Transfer Ideal plasmid transfer
Emergence of MBLs in the United States WA CA CA WA CA CA WA MN MD CA IL VA First KPC CA CA CA IL MA 2001 2009 2010 2011 NDM IMP VIM Yigit et al. 2008. AAC MMWR. 2010. June MMWR. 2010. Sep Mochon et al. 2011. JCM Limbago et al. 2011 submitted Slide courtesy of A. Kallen, CDC
What is Public Health Doing? • CDC • Monitoring voluntary reports by states • Conducting active population-based surveillance of selected organisms in EIP – MN, GA, OR; CO and MD joining • Incidence rates and disease burden • Mechanisms of resistance • Transmission from other countries • Providing education tools and guidelines • CDPHE • Joining CDC active surveillance in EIP Denver metro area • Working with IPs and microbiology laboratories • General consensus - will make select organisms reportable statewide • Will provide education and guidance to facilities with their first CRE or those experiencing transmission of CRE
Carbapenem-Resistant Enterobacteriaceae(CRE) • Cases to be reported within 7 days statewide • Purposes of reporting • Track numbers of cases and rates statewide in Colorado, and report regional and state data • Collect data in Denver metro for national surveillance project • Detect outbreaks • Provide education and guidance • Help facilities stop transmission • Detect community onset cases and cases with unusual features
Carbapenem-Resistant Acinetobacterbaumanii(CRAB) • Cases to be reported within 30 days in the Denver metropolitan area (from sterile sites or urine specimens only) • Purposes of reporting • Track numbers of cases and rates in the Denver metropolitan area over time • Collect data from the Denver-metropolitan area for national surveillance project
Proposed Definitions Escherichia coli, Klebsiella species, and Enterobacter species that are intermediate or resistant to at least one carbapenem (including imipenem, meropenem, doripenem, or ertapenem) AND resistant to all third-generation cephalosporins tested (ceftriaxone, cefotaxime, and ceftazidime); OR Escherichia coli, Klebsiella species, and Enterobacter species that test positive for carbapenemase production (by any method, including the Modified Hodge Test, disk diffusion, or PCR) Acinetobacterbaumannii (including Acinetobacterbaumannii complex and Acinetobacterbaumannii-calcoaceticus complex) that are intermediate or resistant to at least one carbapenem (including imipenem, meropenem, doripenem, or ertapenem) isolated from a normally sterile site or urine (30 day timeframe for reporting)*
Guidance for control of CRE http://www.cdc.gov/hai/organisms/cre/cre-toolkit/index.html
Labs should promptly notify facilities when CRE is detected
MDROs in LTCFs • Use antibiotics judiciously • Use facility-specific susceptibility data • Consider the individual patient’s situation and prevalence or incidence of MDRO in the facility when considering contact precautions • Patient’s level of functionality • Patient’s ability to have good hand hygiene • Site of infection/colonization • Single rooms when available, or cohort patients if possible http://www.cdc.gov/hicpac/mdro/mdro_0.html
HAI Outbreaks • Healthcare facilities - examples • Hospitals • Ambulatory surgery centers • Outpatient clinics • Dialysis facilities • Pathogens that are typically found in healthcare facilities • Example outbreaks • Salmonella in a NICU • Acinetobacter in a prison • Group A strep surgical site infections • MRSA in a sports team ALL outbreaks in healthcare facilities are reportable to the state health department
Contact information Wendy Bamberg, MD Medical Epidemiologist for Healthcare-Associated Infections Communicable Disease Epidemiology Program Colorado Department of Public Health and Environment wendy.bamberg@state.co.us 303-692-2491
Country-wide KPC outbreak –Israel, 2005-2008 2006: Multiple outbreaks of carbapenem-resistant K. pneumoniaeat multiple Israeli hospitals Feb 2007: Meeting of astute IPs spread occurring nation-wide Clin Infect Dis 2011;52(7):848-55.
Country-wide KPC outbreak –Israel, 2005-2008 Interventions: Mandatory reporting of CRE to public health Mandatory isolation of all carriers Creation of national Task Force on Antimicrobial Resistance and Infection Control Clin Infect Dis 2011;52(7):848-55.
Country-wide KPC outbreak –Israel, 2005-2008 Clin Infect Dis 2011;52(7):848-55.
Country-wide KPC outbreak –Israel, 2005-2008 The greater the number of CRE carriers hospitalized (prevalence), the higher the incidence of new acquisitions For each hospitalized carrier, the incidence increased by 0.43 For each increase of 10% in compliance, there was a decrease in incidence of 0.6 cases per 100,000 patient-days Clin Infect Dis 2011;52(7):848-55.
Country-wide KPC outbreak –Israel, 2005-2008 High nation-wide compliance due to: Centrally coordinated IC interventions Mandatory guidelines Daily monitoring by the task force of degree of compliance at all hospitals Hospital director responsible for containment Immediate feedback on compliance Visits by the task force every year and during outbreaks Dedication to IC by healthcare providers Clin Infect Dis 2011;52(7):848-55.
Country-wide KPC outbreak –Israel, 2005-2008 ~ “Because of the absence of a national detection system for emergence or spread of drug-resistant bacteria, the nationwide character of the outbreak went unnoted for over a year without concerted intervention. Although the outbreak was confronted at the local hospital level during 2006, containment was achieved only after national-level intervention.” ~ Clin Infect Dis 2011;52(7):848-55.