Download
1 / 61
620 likes | 1.06k Views
Hyponatremia 2010. Robert M. Centor, MD. Goals. Learn a standardized method for diagnosing hyponatremia Learn how to treat acute CNS complications from hyponatremia Learn how to prevent demyelination syndromes associated with hyponatremia correction. Diagnosis – Step #1. Prove hyponatremia

E N D
Hyponatremia 2010 Robert M. Centor, MD
Goals • Learn a standardized method for diagnosing hyponatremia • Learn how to treat acute CNS complications from hyponatremia • Learn how to prevent demyelination syndromes associated with hyponatremia correction
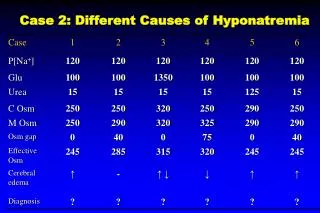
Diagnosis – Step #1 • Prove hyponatremia • Repeat labs • Check serum osms • Pseudohyponatremia 2010 • Hypertriglyceridemia • Paraproteinemia • Mannitol or glycine • Special case – hyperglycemia
Hyperglycemia and HypoNa • 2 commonly used osm equations consistently underestimated measured osms • To assess serum osms in hyperglycemic pts measure the osms
Basic rule of hyponatremia • In clinical practice, it is most useful to consider that cases of abnormal ECF sodium concentration are due to problems with the water control mechanisms. – page 13
Diagnosis – Step #2 • Assess volume status • Edematous states are generally not a problem • Diagnosing volume contraction is often difficult • Fractional excretion of urea • IVC ultrasound
Edematous states • Heart failure – very bad prognostic sign • Cirrhosis – very bad prognostic sign • Concept of decreased arterial volume
Volume contraction • Appropriate ADH response • Water intake without sufficient solute • Corrects easily with saline
Special risk - pre-menopausal women • Increased ADH release to any stimulus • Classic examples • marathon running • Post-op
Euvolemic • Check urine osms
Case #1 • A 32 YO woman brought to the hospital with altered mental status and seizures. H/O beer binge Laboratory data:
Case #1 • A 32 YO woman brought to the hospital with altered mental status and seizures. H/O beer binge Laboratory data: Sosm 250, Uosm 45
Dilute urine and hypoNa • Psychogenic polydipsia • Beer potomania • Tea and toast
Understanding beer potomania • Each liter of urine requires 50 mOsm of solute • Beer contains less than 50 mOsm • Thus, unless you eat the nachos (or pizza or pretzels), you can retain water • Same idea with tea and toast diet
Corollary • If we modestly impair dilution, then a “borderline” tea and toast patient may become hypoNa
Define dilute • Classic definition < 100 • Recent paper suggests considering < 200
Case #2 • A 47 YO man presents with empyema, weakness and low serum sodium Laboratory data:
Case #2 • A 47 YO man presents with empyema, weakness and low serum sodium Laboratory data: Sosm 234, Uosm 324
Surprise finding • TSH 26.8 • Free T4 < 0.023 • Free T3 = 1.16 • Patient responded to thyroid supplementation with remarkable clinical improvement
Exclude these when urine not dilute • CKD – decreased concentration and dilution • Thiazides – decreased dilution • Hypothyroidism – inability to suppress ADH (probably secondary to decreased cardiac output) • Glucocorticoid deficiency – leads to increased ADH
Stimuli for ADH release • Post-op – pain, stress, nausea • Volume contraction • Drugs • Opiates • SSRIs • Other CNS drugs • Pulmonary diseases • CNS disease
SIADH • Some include examples from previous slide • ADH production from a tumor
Diagnosis summary • Confirm hyponatremia • Assess volume • If euvolemic – check urine osms • If dilute – limited differential • If concentrated • Look for reversible ADH stimulus • If not reversible, diagnose SIADH
Combinations • Polydipsia, beer potomania or tea/toast • +++ • Impaired dilution or ADH stimulation
Case #3 • 82-year-old AA man, with history of dementia, hypertension and PEG tube nutrition • Recent discharge from ER for AMS secondary to hypernatremia • Now 4 days of worsening mental status
Lab data • Serum sodium 113 • serum creatinine 1.7; eGFR = 50 • Serum osm 257; urine osm 141
Further history • At hypernatremia visit, daughters received instructions to increase the amount of water with PEG feedings • So they increased to 3-4 liters daily
What happened • CKD causes inability to maximally dilute urine • Water intake exceeded his ability to excrete free water
Case #4 • A 60 YO schizophrenic woman brought to the hospital because of a seizure Laboratory data:
Additional history • Pt. recently moved to Alabama from Indiana • Known schizophrenia and depression • Sisters say she has been compulsively drinking water • No known previous seizures
Additional lab data • Urine osm – 350
Medications • Nefazodone (Serzone) • Olanzapine (Zyprexa)
Diagnosis • Increased ADH – secondary to her SSRI • Exacerbated by polydipsia (despite olanzapine)
Outpatient hyponatremia • The myth of asymptomatic hyponatremia
Asymptomatic hyponatremia • Sodium 115 - 132 • Not truly asymptomatic • Odds ratio for falls – 67! • Careful testing shows • Decreased attention • Unstable gait • Changes > mild alcohol intake
Acute hyponatremia treatment • Seizures • Altered mental status • Neurogenic pulmonary edema
Treatment of acute hyponatremia • Indications for very aggressive treatment • Active seizures • Respiratory failure • Indications for aggressive treatment • Seizures (not active) • Decreased mental status • Headache, nausea and vomiting
Very aggressive treatment for hyponatremia • Bolus 100 cc of 3% NaCl over 10 minutes • Can repeat 1 or 2 times until clinical improvement or Na increased 2-4 mEq/l • Then start aggressive treatment
Aggressive treatment for hyponatremia • 3% NaCl at rate 1cc/kg/hr • Stop infusion when symptoms relieved • Check serum sodium every 2 hours • Avoid sodium increase of greater than 15-20 mEq/l over 48 hours • Slow down at Na = 125-130 mEq/l • Immediate rate is not important – rate over 48 hours represents risk for demyelination
Reference for treatment • Dysnatremias: Why Are Patients Still Dying? • Achinger SG, Moritz ML, Ayus JC
Case #5 Why not saline? • Patient with a sodium = 125. • Serum osms = 249. • Volume = euvolemic. • Prior to urine osm, started IV saline (1.3 L)
This is why not saline • Urine osm = 630 • Serum sodium dropped to 118
Explanation • 1 liter of saline has 300 mOsm of solute • urine = 600 mOsm/liter. • 300 mOsm of NaCl with a urine = 600 mOsm/liter = 500 cc of urine. • Thus, we divide a liter of saline into 500 cc of 600 mOsm/L urine and 500 cc of water. • i.e. giving saline actually provides free water
Assumptions: Na 120, Sosm 250 mOsm/L, Uosm 600 mOsm/L 500 cc of urine ~600 mOsm/L 1000 cc ofNS, ~300 mOsm/L 500 cc of water
Case #6 - The importance of slow • 52 yo alcoholic woman – ER w/ seizures • Na = 96 • Three 100cc boluses of 3% saline • Seizures resolved • Then normal saline • 24 hours later – Na = 128 • MRI – central pontine myelinosis
Mistakes • Too many handoffs • Sodium not checked frequently • Once seizures stop – check Na and switch to D5/W to prevent rapid increase • OR
Avoiding rapid increase • Classic approach • Check labs every 2 hours • Switch to either D5/W or ½ NS if sodium increasing too quickly • New approach • A case
Case #7 • A 45-year-old alcoholic man found unresponsive. Recently started on hctz and SSRI Laboratory data:
Demyelination syndromes • Classic patient at risk • Patient had: • Thiazide • SSRI • Beer potomania (by history) • Alcohol withdrawal • Volume contraction • Raise sodium VERY SLOWLY
A new approach • Goal – 6 mOsm per day • 3% NS when needed • Desmopressin to prevent urine dilution