Download
1 / 118
0 likes | 2 Views
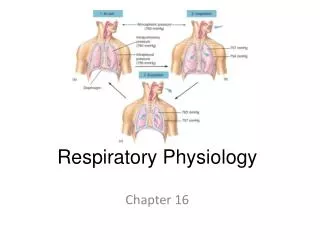
PHYSIOLOGY OF RESPIRATION DURING ANESTHESIA

E N D
APPLIED RESPIRATORY PHYSIOLOGY DURING ANESTHESIA HOSSAM ATEF ; MD Assistant professor Department of Anesthesiology and Critical Care
Factors Dealing With Respiratory Function • Gravity-Determined Distribution of Perfusion , ventilation perfusion - ventilation- V/Q ratio • Non-gravitational factors of PVR & blood flow distribution • Passive process : cardiac out put – lung volumes • Active process: 1) local tissue derived products 2) alveolar gas concentrations 3)neural influences 4)humoral (hormonal) • Other nongravity- factors of compliance – resistance – volume - ventilation
Gravity factors of Perfusion , ventilation • Perfusion ZONE 1 ( Collapse ) PA>Ppa>Ppv ZONE 2 (Waterfall ) Ppa>PA>Ppv ZONE 3 (Distention ) Ppa>Ppv>PA ZONE 4 (Interstitial pressure ) Ppa>Pisf>Ppv>PA
Lung zones • Zone 1, where alveolar pressure is higher than arterial or venous pressure; • Zone 2, where the alveolar pressure is lower than the arterial but higher than the venous pressure. • Zone 3, where both arterial and venous pressure is higher than alveolar.
Zone 4;at the lung bases at low lung volumes or in pulmonary edema. Pulmonary interstitial pressure (Pi) rises as lung volume decreases due to reduced radial tethering of the lung parenchyma. • Pi is highest at the base of the lung due to the weight of the above
ZONE 1 • Collapse & Alveolar dead space 1) Ppa (SHOCK) 2)PA (Vt & peep ) • Normally little or no zone 1 exists in the lung
ZONE 2 (cyclic circulation) • Waterfall ,Weir ,Sluice ,Starling resistor • Cyclic circulation • Flowrate becomes independent of downstream pressure once the flow becomes limited (i.e., the waterfall effect).
ZONE 3 (blood zone) • Distention of vessels (gravity) • Circulation is continuous & perfusion pressure (Ppa-Ppv) is constant • Proximal to distal increasing : transmural distending pressure (Ppa-Ppl,Ppv-Ppl) , blood flow • Vascular resistance decreases • The most blood flow is in this zone
ZONE 4 (interstial pressure) • Interstitial pressure • Below the vertical level of left atrium • Pisf > Ppv & perfusion is based on Ppa-Pisf • Conditions resembling zone 4: • PVR : Volume overload, Emboli , mitral stenosis • Negative Ppl : vigorous breathing, airway obstructions( most common: laryngospasm) • Rapid re expansion of lung
VENTILATION • PA is constant in the lung • Ppl increases from apex to bottom (0.25 cmH2O Each cm) • Density of lung is ¼ of water • ∆P Is 7.5 cmH2O apex to bottom (30/4) • Apical Alveoli are 4 fold bigger than the base so most of the Vt goes to basilar alveoli
Ventilation-Perfusion Ratio • Both Ventilation (VA) and Blood flow (Q) increase linearly with distance down the lung • Blood flow increases more ( VA/Q <1 in the base) • Base is hypoxic & hypercapnic • Because of rapid co2 diffusion ∆P o2> ∆Pco2 apex to base (4 fold)
Non-gravitational factors of PVR & blood flow distribution • PASSIVE PROCESSES: • Cardiac output: Pulmonary vascular system is high flow and low pressure so : QT increases more than Ppa & PVR=Ppa/QT so: PVR decreases • Lung volumes: FRC is the volume in witch PVR is minimum , volume increase or decrease from FRC causes PVR increase: • Above FRC : Alveolar compression of small vessels (small vessel PVR) • Below FRC : 1) Mechanical tortuosity of vessels (passive) 2) Vasoconstriction (main mechanism) (active)
Non-gravitational factors of PVR & blood flow distribution • ACTIVE PROCESSES: 1.local tissue derived products 2.alveolar gas concentrations 3.neural influences 4.humoral (hormonal)
1-Local tissue factors • From Endothelial – Smooth muscle 1) NO : three forms neural , inducible , endothelial predominant endogenous vasodilator compound has small size , freely diffuses , increases cGMP, vasodilatation 1) cNOS (constitutive): Permenantly exists, short bursts of NO ( ca , calmodulin) , keeps PVR low 2) iNOS (inducible) : Inflamation , large quantities & extended duration
Local tissue factors • From Endothelial – Smooth muscle 2) Endotheline: - ET-1 is the only endotheline that is made in lungs (vasoconstriction) • ET receptors: 1) ET A vasoconstriction 2) ET B vasodilatation (NO, prostacyclyn)
Local tissue factors • Vasoactive products: 1) Adenosine Vasodilatation 2) NO Vasodilatation 3) Eicosanoids a)PGI2 (Epoprostenol , Iloprost) Vasodilatation b)Thromboxane A2 Vasoconstriction c)Leukotriene B4 Vasoconstriction 4)Endotheline Vasoconstriction & Vasodilatation
2-ALVEOLAR GASES • Hypoxemia • Causes localized pulmonary vessel vasoconstriction (HPV) • Causes systemic blood vessel vasodilatation • HPV • Vessels near small bronchioles • PSO2 : Oxygen tension at HPV stimulus site that is related to PAO2 & PvO2 (PAO2 Has much greater effect) • PSO2-HPV Response is sigmoid : 50% response at PSO2=PAO2=PvO2=30 mmHg
CAUSES OF HPV • Alveolar hypoxia pulmonary vascular smooth muscle ETC change H2O2 (2nd messenger) Ca Vasoconstriction • Epithelial & smooth muscle derived products • Hypercapnia • Acidosis (metabolic & respiratory)
CLINICAL EFFECTS OF HPV • Life at high altitude (FIO2 Ppa zone1 zone2 PaO2 ) • Hypoventilation – Atelectasis – Nitrogen ventilation (HPV Shunt ) • Chronic lung disease (asthma-MS-COPD) administration of pulmonary vasodilator drugs (TNG-SNP-IPN) Transpulmonary shunting PVR & PaO2
3-NEURAL EFFECT • Sympathetic system ( α1 effect is predominant ) • Parasympathetic system ( VAGUS nerve ) ,NO-dependent , vasodilatation acetylcholine binds M3 muscarinic receptor ↑↑ Ca ↑ cNOS • NANC system NO-dependent vasodilatation using vasoactive intestinal peptide as neurotransmitter
4-HUMORAL EFFECTS • Vasodilator :histamine ( H1 on endothelium-H2 on smooth muscle) , adenosine , bradykinin , substance P • Vasoconstrictor :histamine (H1 on smooth muscle), neurokinin, angiotensin, serotonin • Normalizer : ATP
NON ALVEOLAR PATHWAYS OF BLOOD FLOW THROUGH THE LUNG • FRC< CC Atelectasis Right to left shunting • Normal shunting : 1- 3% of cardiac out put (plural & bronchial circulation) • Chronic bronchitis : 15% of cardiac out put • PFO : 20-30% of individuals • Any condition that causes right atrial pressure to be greater than left atrial pressure may produce right to left shunting : pulmonary emboli, COPD, CHF, PS, High peep, Emergence • TEE is the most sensitive test for detecting PFO in anesthetized patients
Other nongravitational factors of compliance – resistance – volume - ventilation • COMPELIANCE C L/cm H2O= ∆V/ ∆P • 1/CT=1/CL + 1/CCW CT = CLX CCW/CL+CCW • Normally , CL=CCW=0.2 SO CT= 0.1 • In clinic only CT can be measured • CT 1) Dynamic ∆P/ peak pressure 2) Static ∆P/plateau pressure • Peep must first subtracted from the peak or plateau pressure
LAPLACE expression : P = 2T / R • T (surface tension) • R( radius of curvature of the alveolus) • Surfactant secreted by the intra alveolar type ║ T lipoprotein
Airway resistance • R = ∆P/ ∆V • R (Resistance) cmH2O/L/sec • V ( airflow) L/sec • ∆P along the airway depends on the caliber of the airway & pattern of airflow
Patterns of airflow • LAMINAR : Gas passes down a parallel sided tube at less than a certain critical velocity • TURBULENT: when flow exceeds the critical velocity becomes turbulent • ORFICE : occurs at severe constrictions (kinked ETT, laryngospasm) the pressure drop is proportional to the square of the flow Laminar flow is confined to the airways below the main bronchi, flow in trachea is turbulent , & orifice flow occurs at the larynx 6 factors pressure, radius, resistance, length, viscosity, density
Time constant • One time constant represents the time required for the respiratory system to reach 63% of its equilibrium value and is an indication of the time required for the lungs to empty during exhalation. • ƬE was estimated from 0.10 to 0.50 seconds after the beginning of exhalation.
Time constant τ=C×R • Raw = (PIP – Pplat) • Time Constant = (Raw / flow L/cmH20) • Expiratory time = Time Constant x 3 Example: 3 converted to 0.3 • The expiratory time constant (RCEXP), the product of airway resistance and lung compliance
Time constant • Enable us to assess the mechanical properties of the respiratory system in mechanically ventilated patients. • Although RCEXP could also be applied to spontaneously breathing patients • Longer than approximately 0.6 s can be linked to the presence of airway obstruction.
DIFFERENT REGIONAL LUNG TIME CONSTANTS • זּ =CTX R • זּ (time constant) is the time required to complete 63% of an exponentially changing function (2זּ = 87% ,3 זּ= 95% ,4 זּ=98%) • CT = 0.1 ,R= 2 so זּ=0.2 sec 4 זּ=0.8 sec • Time increases as resistance or compliance increases
Pathway of collateral ventilation • Non gravitational • Are designed to prevent hypoxia in neighboring • Interalveolar communications (kohn pores) • Distal bronchiolar to alveolar (lambert channels) • Respiratory bronchiole to terminal bronchiole (martin channels) • Interlobar connections
WORK OF BREATHING • Work=force x distance, Force=pressure x area, Distance=volume/area • So WORK = PRESSURE x VOLUME • If R or C ,P , Work • The metabolic cost of the work of breathing at rest is only 1-3% of the total O2 consumption , and increases up to 50% in pulmonary disease • Expiration is passive using potential energy that has been saved during inspiration (awake) • In anesthetized person with diffuse obstructive airway disease resulting from the accumulation of secretions, elastic and airway resistive component of respiratory work would increase • For a constant minute volume , both deep , slow (elastic resistance ) & shallow , rapid (airway resistance ) breathing will increase work of breathing
LUNG VOLUMES • FRC: the volume of gas in lung at end of normal expiration • At FRC , There is no air flow & PA = ambient pressure • Expansive chest wall elastic forces are exactly balanced by retractive lung tissue elastic forces • ERV: is part of FRC, the volume of gas that can be consciously exhaled • RV: the minimum volume that remains after ERV • VC: ERV + IC IC : VT+ IRV TLC: VC+ RV • Total lung capacity; the total volume of air in the lungs at full inhalation; the sum. of all volume compartments (IC + FRC or IRV + VT + ERV + RV) (L)
LUNG VOLUMES • Volumes that can be measured by simple spirometry are VT , VC , IC , IRV ,ERV • TLC ,FRC & RV cannot be measured by spirometry • How to measure TLC ,FRC & RV : • Nitrogen wash out • Inert gas dilution • Total body plethysmography • Disparity between FRC in 2&3 is used to detect large nonventilating airtrapped blebs
Nitrogen wash out • The patient breathes 100% oxygen and breathes out into a spirometer, with monitoring of the nitrogen in the expired gas until all is washed out. • (a) an estimate of anatomical dead space; (b) an assessment of the distribution of ventilation, and (c) a measure of closing volume
Inert gas dilution • Gas dilution is a method of determining those lung volumes that cannot be determined from simple spirometry. • These include FRC, which is computed directly, and RV and TLC, which are computed from FRC • Reducing the oxygen content in the tank by diluting the air with inert gas containing less than 5% oxygen by volume.
Plethysmography • Three types of plethysmographs: pressure, volume, and pressure-volume • Uses Boyle's law in order to measure the intrathoracic gas volume or functional residual capacity • The measurement of TLC is necessary for the diagnosis of restrictive diseases.
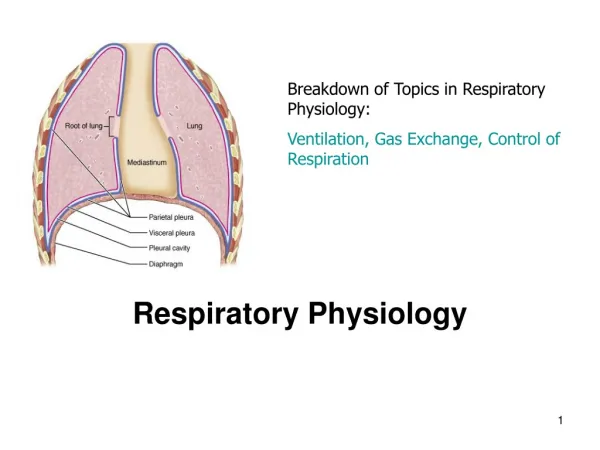
Airway closure & closing capacity • Ppl (pleural pressure) increases from top to the bottom and determines alveolar volume, ventilation & compliance • Gradients of Ppl may lead to airway closure and collapse
Airway closure in patients with normal lung • In normal resting end expiratory state (FRC) , the distending transpulmonary exceeds intrathoracic air passage transmural pressure and the airways remain patent • During the middle of normal inspiration ∆P increases and the airways remain patent • During the middle of normal expiration ,expiration is passive and PA is related to elastic recoil of the lung, airways remain patent
4. During the middle of forced expiration , Ppl increases more than atmospheric pressure, in alveoli because of elastic recoil of alveolar septa, pressure is higher than Ppl, pressure drops down as air passes to the greater airways, and there be a place at which intraluminal pressure equals Ppl (EPP), down stream this point (small or large airways) air way closure will occur • Distal to 11th generation there is no cartilage=bronchioles • Airway patency below this point is due to lung volume above this point is due to intra thoracic pressure
If lung volume decreases EPP goes downward (closer to alveolus ). • Near RV small airways (<0.9mm) tend to close • Airway closure first happens in dependent lung regions (Ppl> Pintraluminal)
Airway closure in abnormal lung • EPP Is lower, airway closure occurs with lower gas flow, and higher lung volume R ,Flow , Air way Radius • Emphysema: Elastic recoil • Epp is close to alveoli , transmural ∆p can become negative • Epp is very near to point of collapse • Bronchitis: Weak airway structure that may be closed with little negative transmural ∆p • Asthma: Bronchospasm narrow middle size airways forced expiration closure • Pulmonary Edema: peri bronchial & alveolar fluid cuffes alveolus &bronchi FRC , CC
CC: Is the amount of gas that must be in the lunges to keep the small conducting airway open & is = RV+ CV • CC : Smoking , obesity , aging , supine position 44 years CC = FRC in supine position 66 years CC = FRC in upright position
Relationship Between FRC & CC • CC >> FRC Atelectasis (CC > VT) • CC > FRC Low VA/Q (CC is in VT) volume dependent • FRC > CC Normal • Intermittent positive pressure breathing: • In awake individual increases Inspiratory time & increases VA/Q • In anesthetized patients (Atelectasis in dependent Area) patient’s lung will not be reserved • If peep is added → FRC → FRC > CC no closure
Oxygen & carbon dioxide transport • Two thirds of each breath reaches alveoli • The remaining third is termed physiologic or total dead space VDphy = VDAna +VD Alv • physiologic dead space: • Anatomic dead space (airway) 2 cc/kg • Alveolar dead space (zone 1- emboli) upright 60-80 cc supine VDphy = VDAna (VD Alv= 0)
Naturally Vco2(co2 entering the alveoli) is equal to the co2 eliminated • Vco2 = (VE)(FE co2) • Expired gas = alveolar gas + VD gas • So Vco2 = (VA)(FA co2)+(VD)(FI co2) • Modified bohr equation : VD/VT=(Pa co2 – PE co2) / Pa co2 • In a healthy adult VD/VT < 30% • In COPD VD/VT > 60%
Alveolar air • Alveolar air contains much more water vapor (6.2 percent) and carbon dioxide (5.3 percent), resulting in a dilution of nitrogen to 74.9 percent • PAO2=(PB−PH2O)FiO2−(PaCO2÷R)where PB is the barometric pressure, PH2O is the water vapor pressure (usually 47mmHg), and R is the gas exchange ratio 4.9 percent and oxygen to 13.6 percent.
Alveolar gas concentration = FI gas – out put/alveolar vent. PA gas = FI gas + V gas / VA • P dry Atmospheric = P wet Atmospheric – P H20 • 713 = 760 – 47 • PA O2 = 713 X (FIO2 – VO2/VA) • PA CO2=713 X (V co2 /VA) x 0.863 • Fresh gas flow < 4 lit/min PaCO2 ,PA O2
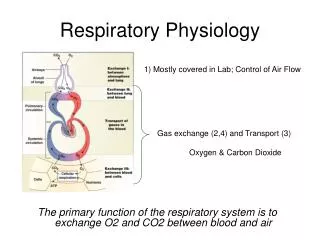
Oxygen Transport • Cardiopulmonary system has the ability to increase function more than 30 folds • Functional links in the oxygen transport chain: • Ventilation • Diffusion of o2 to blood • Chemical reaction of o2 with Hb • QT of arterial blood • Distribution of blood to tissue and release of o2
Oxygen-hemoglobin dissociation curve • Hb molecule consists of four heme molecule attached to a globin molecule • Each heme molecule consist of : • glycine , • α-ketoglutaric acid • Iron in ferrous form ( ++ ) • Hb is fully saturated by a PO2 of about 700 mm Hg • This curve relates the saturation of Hb to PaO2 • PaO2 = 90 -100 SaO2=95-98 • PaO2 = 60 SaO2=90 • PVO2 = 40 SVO2 =75