Download
1 / 48
490 likes | 853 Views
The Management of Acute Respiratory Distress Syndrome. 署立桃園醫院 胸腔內科 林倬睿醫師. Outlines. Introduction Ventilator strategy Adjunctive therapy Case demonstration. 定義 Definition. 急性 Acute onset 缺氧 PaO2/FiO2 < 200 mmHg CXR: bilateral infiltrates 雙側浸潤

E N D
The Management of Acute Respiratory Distress Syndrome 署立桃園醫院 胸腔內科 林倬睿醫師
Outlines • Introduction • Ventilator strategy • Adjunctive therapy • Case demonstration
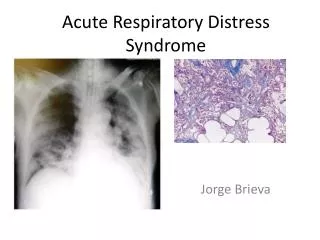
定義 Definition • 急性 Acute onset • 缺氧 PaO2/FiO2 < 200 mmHg • CXR: bilateral infiltrates雙側浸潤 • 排除心因性呼吸衰竭 PAWP < 18 mmHg, no clinical evidence of LA HTN
致病原因 • Direct injury • Pneumonia • Gastric aspiration • Drowning • Fat and amniotic fluid embolism • Pulmonary contusion • Alveolar hemorrhage • Toxic inhalation • Reperfusion • Indirect injury • Severe sepsis • Transfusions • Shock • Salicylate or narcotic overdose • Pancreatitis
Differential Diagnosis • Left ventricular failure • Intravascular volume overload • Mitral stenosis • Veno-occlusive disease • Lymphangitic carcinoma • Interstitial and airway diseases • Hypersensitivity pneumonitis • Acute eosinophilic pneumonia • Bronchiolitis obliterans with organising pneumonia Lancet 2007; 369:1553-65
Prognosis & Outcome • Predictive of death: advanced age, shock, hepatic failure • Overall 28-day mortality: 20-40% • Lung function: returns to normal over 6-12 months • Common complications: neuropsychiatric problems, neuromuscular weakness Lancet 2007; 369:1553-65
Pathophysiology • Exudative phase • Cytokines inflammation surfactant dysfunction atelectasis • Elastase epithelial barrier damage edema • Procoagulant tendency capillary thrombosis • Fibroproliferative phase • Chronic inflammation • Fibrosis • neovascularisation Lancet 2007; 369:1553-65
Treatment • No specific treatment • Mainstay of treatment: supportive care • Avoid iatrogenic complications • Treat the underlying cause • Maintain adequate oxygenation
Supportive Care • Prevention of deep vein thrombosis, gastrointestinal bleeding, and pressure ulcers • Semi-recumbent position • Enteral nutrition • Infection control • Goal-directed sedation practice • Glucose control
Barotrauma Volutrauma Atelectrauma Biotrauma Ventilator-induced Lung Injury (VILI) Over Distension Collapse
Volutrauma • Increased alveolar wall stress (stretch) by high tidal volume • Parenchymal injury • Gross physical disruption • Stretch-responsive inflammatory pathways AJRCCM 1998; 157: 294-323
Lung edema PEEP PEEP PEEP Atelectrauma • Cyclic closing and reopening of alveoli • Alveolar shear stress-related injury • Heterogeneous nature of lung aeration in ALI/ARDS
The PEEP Effect NEJM 2006;354:1839-1841
Ventilator-induced Lung Injury (VILI) Upper Deflection point Lower Inflection point
Lung-Protective Ventilation ARDS Network, 2000: Multicenter, randomized 861 patients NEJM 2000; 342: 1301-1308
Lung-Protective Ventilation • Result: • Lower 22% mortality (31% vs 39.8%) • Increase ventilator-free days NEJM 2000; 342: 1301-1308
Concerns when using lung-protective strategy… • Heterogeneous distribution • Hypercapnia • Auto-PEEP • Sedation and paralysis • Patient-ventilator dyssynchrony • Increased intrathoracic pressure • Maintenance of PEEP
Other Ventilator Strategies • Lung recruitment maneuvers • Prone positioning • High-frequency oscillatory ventilation (HFOV)
Lung Recruitment • To open the collapsed alveoli • A sustained inflation of the lungs to higher airway pressure and volumes • Ex.: PCV, Pi = 45 cmH2O, PEEP = 5 cmH2O, RR = 10 /min, I : E = 1:1, for 2 minutes NEJM 2007; 354: 1775-1786
Lung Recruitment NEJM 2007; 354: 1775-1786
Lung Recruitment NEJM 2007; 354: 1775-1786
Lung Recruitment • Potentially recruitable (PEEP 5 15 cmH2O) • Increase in PaO2:FiO2 • Decrease in PaCO2 • Increase in compliance • The effect of PEEP correlates with the percentage of potentially recruitalbe lung • The percentage of recruitable lung correlates with the overall severity of lung injury Sensitivity : 71% Specificity : 59% NEJM 2007; 354: 1775-1786
Lung Recruitment • The percentage of potentially recruitable lung: • Extremely variable, • Strongly associated with the response to PEEP • Not routinely recommended
Prone Position • Mechanisms to improve oxygenation: • Increase in end-expiratory lung volume • Better ventilation-perfusion matching • More efficient drainage of secretions
Prone Position NEJM 2001;345:568-573
Prone Position NEJM 2001;345:568-573
Prone Position • Improve oxygenation in about 2/3 of all treated patients • No improvement on survival, time on ventilation, or time in ICU • Might be useful to treat refractory hypoxemia • Optimum timing or duration ? • Routine use is not recommended
HFOV Frequency: 180-600 breaths/min (3-10Hz)
Effect of HFOV on gas exchange in ARDS patients AJRCCM 2002; 166:801-8
Survival difference of ARDS patients treated with HFOV or CMV 30-day: P=0.057 90-day: P=0.078 AJRCCM 2002; 166:801-8
HFOV • Complications: • Recognition of a pneumothorax • Desiccation of secretions • Sedation and paralysis • Lack of expiratory filter • Failed to show a mortality benefit • Combination with other interventions ? Chest 2007; 131:1907-1916
Adjunctive Therapy • Steroid treatment • Fluid management • Extracorporeal membrane oxygenation (ECMO) • Nitric oxide • Others
Steroid therapy NEJM 2006;354:1671-1684
Steroid therapy • Increase the number of ventilator-free and shock-free days during the first 28 day • Improve oxygenation, compliance and blood pressure • No increase in the rate of infectious complications • Higher rate of neuromuscular weakness • Routine use of steroid is not supported • Starting steroid more than 14 days after the onset of ARDS may increase mortality NEJM 2006;354:1671-1684
Fluid Management NEJM 2006;354:2564-2575
Fluid Management NEJM 2006;354:2564-2575
Fluid Management NEJM 2006;354:2213-24
Fluid Management • Conservative strategy improves lung function and shortens the duration of ventilator use and ICU stay • No significant mortality benefit • The use of pulmonary artery catheter not routinely suggested
Extracorporeal Membrane Oxygenation (ECMO) • No improvement on survival or time on ventilation • Substantial risk of infection and bleeding • Not routinely recommended
Nitric Oxide • Vasodilator • Improve oxygenation and pulmonary vascular resistance • No improvement on survival • Routine use is not recommended
Unproven Treatments • Ketoconazole • Pentoxyfilline and lisofylline • Nutritional modification • Antioxidants • Neutrophil elastase inhibition • Surfactant • Liquid ventilation Lancet 2007; 369:1553-65
Conclusions • The only treatment that shows mortality benefit: • lung-protective ventilation strategy • Low tidal volume (6ml/Kg), high PEEP, adequate Pplat (<30 cmH2O) • Modalities to improve oxygenation: • Prone position, steroid, fluid treatment, steroid, HFOV, NO • Combining other treatments: • Activated protein C, antibiotics, EGDT…etc