Download
1 / 36
360 likes | 433 Views
Acute Respiratory Distress Syndrome. Christopher B. Powe, PhD, ACNP-BC Principle | Global Training Institute. Outline. Outline. Definition Causes (Traumatic Examples) Features Clinical Pathological Radiological Epidemiology Pathogenesis Treatment. Definition.

E N D
Acute Respiratory Distress Syndrome Christopher B. Powe, PhD, ACNP-BC Principle | Global Training Institute
Outline Outline • Definition • Causes (Traumatic Examples) • Features • Clinical • Pathological • Radiological • Epidemiology • Pathogenesis • Treatment
Definition • First description 1967, Ashbaugh and colleagues • Acute Respiratory Distress • Cyanosis Refractory to Oxygen Therapy • Decreased Lung Compliance • Diffuse Infiltrates evident on Chest Radiograph • Initially called Adult Respiratory Distress Syndrome • Changed to Acute (does occur in children)
Definition • 1994 American-European Consensus Conference Committee • Acute Onset • Bilateral Infiltrates on CXR • PAWP < 18 mmHg • Acute Lung Injury: PaO2:FiO2 is > 300 • Acute Respiratory Distress Syndrome: PaO2:FiO2 <200
Causes • Common, devastating injury affecting both medical and surgical patients • Can be caused from direct or indirect injury • Sepsis is associated with highest progression • 40% of patient with ARDS also have Sepsis • Multiple predisposing disorders increase risk • Chronic ETOH abuse, Chronic Lung Disease and Low serum pH
Clinical Features • Three Stages • Acute (Exudative Changes) • Progression to Fibrosing Alveolitis • Recovery
Acute Phase • Clinical • Rapid Respiratory Failure • Refractory Hypoxemia • Bilateral Infiltrates on CXR • Indistinguishable from cardiogenic pulmonary edema • Pathological • Diffuse alveolar damage • Presence of neutrophils, macrophages, erythrocytes, hyaline membrane, and protein rich edema fluid in alveolar spaces, capillary injury and disruption of alveolar epithelium
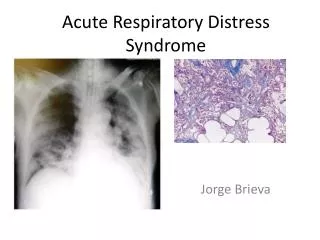
Radiographic and Computed Tomographic (CT) Findings in the Acute, or Exudative, Phase (Panels A and C) and the Fibrosing-Alveolitis Phase (Panels B and D) of Acute Lung Injury and the Acute Respiratory Distress Syndrome Ware, L. B. et al. N Engl J Med 2000;342:1334-1349
Findings on Light Microscopy and Electron Microscopy during the Acute Phase (Panels A and D) and the Fibrosing-Alveolitis Phase (Panels B, C, and E) of Acute Lung Injury and the Acute Respiratory Distress Syndrome Ware, L. B. et al. N Engl J Med 2000;342:1334-1349
Fibrosing Alveolitis Stage • Clinical • Persistent refractory hypoxemia • Increased alveolar dead space • Further decreased compliance • CT Chest shows diffuse interstitial opacities and bullae • Pathological • Fibrosis occurs with acute/chronic inflammatory cells • Partial resolution of pulmonary edema
Recovery Phase • Gradual resolution of hypoxemia and lung compliance • Radiographic abnormalities resolve completely • Histologic resolution of fibrosis not well characterized • Pulmonary function returns to normal
Mechanisms Important in the Resolution of Acute Lung Injury and the Acute Respiratory Distress Syndrome Ware, L. B. et al. N Engl J Med 2000;342:1334-1349
Epidemiology • National Institutes of Health • Incidence 75 per 100,000 population • Mortality Rates • 40-60% • Majority of deaths attributed to sepsis (40%) • MSOF another common comorbidity • Mortality rates decreased from 60-70% as a result of new ventilator technologies
Epidemiology • Factors used to predict mortality risk • Chronic liver disease • Nonpulmonary organ dysfunction • Sepsis • Advanced Age • Initial Indexes of Oxygenation/Ventilation • DO NOT predict outcome • No difference in outcome with P:F of 200/300
Epidemiology • Survival Outcomes • Normal pulmonary f(x) return in 6 – 12 mths • Residual impairment of pulmonary mechanics: • Mild restriction • Mild obstruction • Gas exchange abnormalities • Usually asymptomatic
Pathogenesis • Acute Phase • Two barriers form Alveolar-capillary membrane • Microvascular endothelium • Alveolar epithelium • Influx of Edema Fluid • Protein rich edema fluid fills alveolar air spaces • Caused by endothelial injury and increased vascular permeability • Degree of alveolar epithelial injury important predictor of outcomes
Pathogenesis • Acute Phase • Normal Alveolar Epithelium • Two types of cells • 90% Flat Type I cells – very easily injured • 10% Cuboidal Type II cells – resistant to injury • F(x) surfactant production, ion transport, proliferation and differentiation of type I cell after injury • Primary pathologic condition is: • Loss of epithelial integrity
Pathogenesis • Acute Phase – Loss of Epithelial Integrity • Contributes to alveolar flooding • Disruption of epithelial fluid transport • Impairs removal of edema fluid • Reduces production and turnover of surfactant • Leads to septic shock in patients with bacterial pneumonia • Disorganized or insufficient repair leads to fibrosis
The Normal Alveolus (Left-Hand Side) and the Injured Alveolus in the Acute Phase of Acute Lung Injury and the Acute Respiratory Distress Syndrome (Right-Hand Side) Ware, L. B. et al. N Engl J Med 2000;342:1334-1349
Pathogenesis • Neutrophil-Dependent Lung Injury • Clinical studies suggest neutrophil-mediated injury • Questions whether neutrophilic inflammation is the cause or the result of ARDS • Patients with profound neutropenia develop ARDS • Administration of Granulocyte colony-stimulating factor did not increase incidence of ARDS • Anti-inflammatory agents largely are not effective
Pathogenesis • Pro-inflammatory Conditions • Cytokines • Initiate and amplify the inflammatory response • Macrophage inhibitory factor (MIF) produced by anterior pituitary found in high concentrations of BAL • Increases production of proinflammatory cytokines inteliukin-8 and tumor necrosis factor Alpha- and can override glucocorticoid-mediated inhibition of cytokine secretion • Better understanding of biologic cytokine activity is needed
Pathogenesis • Ventilator-Induced Lung Injury • Older studies suggest oxygen toxicity • Experimental studies suggest volutrauma and high PEEP pressures may also damage alveolar epithelium • Overdistention/Hyperinflation of alveoli • Repeated collapse and reopening of alveoli may initiates the cascade of proinflammatory cytokines • Traditional volumes of 10 to 15 cc/kg thought to have caused much of the VI Lung Injury
Pathogenesis • Other Mechanisms of Injury • Abnormalities of Coagulation System • Abnormalities in Surfactant Production • Gas-exchange Abnormalities
Treatment • Supportive care may contribute to recent decline in mortality • Research underlying causes with emergent treatment of: • Sepsis • Pneumonia • Abdominal Infections • Acute Bleeding (trauma) • Catheter-induced sepsis • Prevention of gastric bleeding and thromboembolism
Treatment • Mechanical Ventilation • Mortality rates with Tv 12-15 cc/kg = 39.8% • Mortality rates with Tv 6 cc/kg = 22% • Positive End-Expiratory Pressure (PEEP) • Increases functional residual capacity • Recruits collapsed alveoli • Use of PEEP at 8 cm/H20 or more • Prone positioning currently being researched • Not shown to be beneficial
Treatment • Fluid and Hemodynamic Management • Animal studies suggest low left atrial pressures correlate with reduction of pulmonary edema • Reasonable Objectives: • Maintain intravascular volumes at lowest levels to maintain perfusion • Use of PA / CVP catheters to monitor hemodynamic status
Treatment • Surfactant Therapy • Surfactant-replacement successful in infants • One study showed no effect on oxygenation, duration of mechanical ventilation or survival • Problems with study: • Delivered by aerosol • Only 5% reached distal air spaces • Preparation of surfactant protein-free phospholipid • Current clinical trials • Tracheal installation and bronchoalveolar lavage
Treatment • Inhaled Nitrous-Oxide and Other Vasodilators • Potent vasodilator • Does not cause systemic vasodilation • Randomized, double-blind studies • Shown no improvement in duration or mortality rates • Current Research • Sodium nitroprusside, hydralazine, prostaglandin E1, prostracyclin
Conclusion • Progress has been made: • Understanding pathogenesis • Epidemiology • New ventilation strategies have decreased mortality by 22% • Large prospective, randomized studies are currently needed
Acute Respiratory Distress Syndrome Christopher B. Powe, PhD, ACNP-BC Principle | Global Training Institute