Download
1 / 54
540 likes | 646 Views
Session Plan. Session Plan. Outline of Discussion. What is the site of depression on the map of MD? {Classification of Mental Disorders}ICD-10-PHC & DSM-4 Why Depression? Size of the problem (Morbidity &Burden of Illness…) When do you consider (suspect) depression?

E N D
Session Plan Session Plan
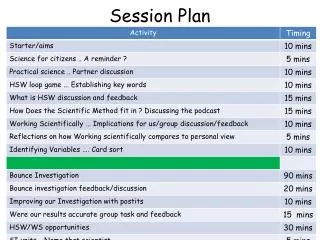
Outline of Discussion • What is the site of depression on the map of MD? {Classification of Mental Disorders}ICD-10-PHC & DSM-4 • Why Depression? • Size of the problem (Morbidity &Burden of Illness…) • When do you consider (suspect) depression? • How do you diagnose a depression? • Clinical presentation and D.D • Tips and Pitfalls in diagnosis of depression? • Management Plan • Risk assessment • Preventive issues related to Mental Disorders.
Patient problem A 34-years-old lady presented to your office, she told you that she has been ‘way down’ for the past 4 months and has not felt much like doing anything. She had a previous “nervous breakdown” when she was 22 years old. She was working as business executive until 4 months ago but has found it impossible not only to work but also to do anything else. She had worked at her present position for approximately 18 months but was finding work an increasing stress. She was working approximately 75 hours/week and having to deal with daily difficulties and conflicts. She is currently on long term sick leave.
She expresses her current situation best by saying, “I have no joy left in life”. I do not enjoy doing anything, I have not any interest in any of my previous activities. Her other symptoms include sleep approximately 14 hours/day, almost continual feelings of guilt and hopeless, a state of having almost no energy “ all of the time” decreased concentrating ability, no appetite and loss of weight + 12 Kg, and being unable to “ move around “ or get anything done. Her marriage is described as “excellent” her husband is very supportive. She does admit, however, to a significant decrease in sexual interest and activity. Her family history is significant for alcoholism in her father. She is on no drug and has no allergies. Her physical examination is completely normal in all systems.
1.What is the most likely diagnosis in this patient? Select the best answer to the following questions A) Adjustment disorder secondary to work stress B) Generalized anxiety disorder C) Major depressive disorder D) Organic affective disorder E) Dysthymia 2.Which of the following types of psychotherapy are most commonly used in the illness above? • Psychoanalytic psychotherapy • Behavioral Psychotherapy • Cognitive psychotherapy • Supportive psychotherapy • All of above
3. The aims or goals of the psychotherapy for this condition include which of the following? • Providing a therapeutic rationale or explanation for the patient's symptoms • Providing ongoing education regarding the illness, prognosis and treatment • Guiding the patient with respect to interpersonal relationships, work, and major life adjustments • Helping to bolster the patient’s morale • All of the above. • 4.What is the pharmacologic agent of choice in the disorder described? • A) a selective serotonin reuptake inhibitor (SSRI) • B) a tricyclic antidepressant • C) a non selective MOA inhibitor • D) a selective MAO inhibitor • E) Lithium carbonate
Patient problem A 41-years old male presents with 3-year history of a “depressed mood”. He states that he feels “depressed most of the time”, although there are periods when he feels better than others. He feels chronically tired, has some difficulty concentrating at work, and has found it difficult to remain productive and efficient as representative of a major company. He has had no other symptoms. His health is otherwise good. He is on no medications.
1) What is the most likely diagnosis? Adjustment disorder Dysthymic disorder Major depressive disorder Organic affective disorder None of the above 2) What is the treatment of choice for this patient? A tricyclic antidepressant Serotinin reuptake inhibitor Supportive and/or cognitive psychotherapy A and C B and C
Answer of the second problem • C • E • E • A Answer of the second problem • B • E
WHEN DO YOU CONSIDER DEPRESSION ? How ? Screening Tool
The common cold” of MD and The “ butter” of psychiatry,
Approach to Pt with Mental Disorders in PHC (Depression) Dr.Nadia Mabrouk A.Prof.FM
Outline of Discussion • What is the site of depression on the map of MD? {Classification of Mental Disorders}ICD-10-PHC & DSM-4 • Why Depression? • Size of the problem (Morbidity &Burden of Illness…) • When do you consider (suspect) depression? • How do you diagnose a depression? • Clinical presentation and D.D • Tips and Pitfalls in diagnosis of depression? • Management Plan • Risk assessment • Preventive issues related to Mental Disorders.
Classification of Mental Disorders (ICD-10-PHC )
WHY DEPRESSION SIZE OF THE PROBLEM • In multi-center worldwide study conducted in 15 countries in general health care screened + 26422 persons using 12-item GHQ, About 25% had well defined mental disorders, further 9% had subthreshold conditions (WHO,1993). • The most common disorders were depression (10%), general anxiety disorder (8%), and harmful use of alcohol (3%)(WHO,1993).
WHY DEPRESSION SIZE OF THE PROBLEM • Lifetime prevalence of major depression (7-12%) among men in epidemiological studies. • Lifetime prevalence of major depression (20-25%) among women in epidemiological studies. • The prevalence of major depression in PHC settings (5-10% )
WHY DEPRESSION SIZE OF THE PROBLEM • Studies demonstrate that one out of seven adult persons in the USA have a mood disorder during a single year, 7% in Brazil, almost 10% in Germany and 4.2% in Turkey. • In the USA, 5% of children aged 9-17 were found to have depression, a disorder thought to spare youth and adolescents. Ignoring this reality can result in suicide.
WHY DEPRESSION SIZE OF THHE PROBLEM IN EGYPT • Prevalence rate of the psychiatric disorders among patients attending primary health care (Ismailia Governorate) using GHQ was 33.5% (Awad, 1985). [The commonest mental disorder was depression (61.5%)]. • Prevalence of psychiatric disorders in rural Egypt was found to be as high as 42.4% in leading community study (El- Akabawy et al.1982). • The prevalence rate of the psychiatric disorders among general population in rural Menia using GHQ was 31.7% (Soliman et al. 1997).[Prevalence rate of depression was 22.8 %& anxiety was 18.6 %& somatization was 18.5%].
WHY DEPRESSION SIZE OF THHE PROBLEM IN EGYPT Eastern Mediterranean Health Journal, Vol. 15, No. 1, 2009 65 National Survey of Prevalence of Mental Disorders in Egypt: preliminary survey M. Ghanem,1 M. Gadallah,2 F.A. Meky,2 S. Mourad3 and G. El-Kholy1
WHY DEPRESSION SIZE OF THHE PROBLEM IN EGYPT • This study was conducted in 2003 as an initial step for the National Survey of Prevalence of Mental Disorders in Egypt. We conducted a door-to-door household survey of 14 640 adults aged 18–64 years in 5 regions in Egypt including Ismailia. • Overall prevalence was estimated at 16.93% of the studied adult population. • The main problems were mood disorders, 6.43%, anxiety disorders, 4.75%, and multiple disorders, 4.72%.
WHY DEPRESSION BURDEN OF ILLNESS CONSEQUENCES OF DEPRESSION • The 1993 world development report of the World Bank estimated that mental health problems represent 8% of the global burden of disease. Its toll is greater than that of TB, cancer or heart disease (World Bank Report, 1993). • It is also responsible for the greatest proportion of burden attributable to non fatal health outcomes, accounting for almost 12% of total years lived with disability
WHY DEPRESSION BURDEN OF ILLNESS CONSEQUENCES OF DEPRESSION • The total annual cost estimate (both direct and indirect costs) is $43.7 billion in the United States • Stigma and QOL • Mortality rate
WHEN DO YOU CONSIDER DEPRESSION Factors which render a person more vulnerable to get depression… examples are: • Positive family history • Loss of mother before the age of 11Y • Cancer in the family • Women with 3 or more children under 14 years of age and living alone, with no close relationship • Post- natal period. • Bereavement, especially widows with no family • Poor diet • Social isolation. Significant life events • Death of a loved one- child, spouse (husband or wife) or a relative. • Divorce or separation • Loss of a job. • Breakdown of a relationship. • Moving house. • Adverse financial conditions. Be biased toward diagnosis of depression
WHEN DO YOU CONSIDER DEPRESSION Difficult consultations • Frequent attendants • Patients with chronic painful physical illness- cancer, diabetes. • Patients with unexplained physical symptoms • Patients with decreased libido Factors that predispose to a new episode of depression or the past history of: • A long history of depression • Manic depressive illness • Sever attack of depression • More than one episode that lasted for more than 2 weeks. Be biased toward diagnosis of depression
How DO YOU Screen for Depression ??????????????????????????????????
DIAGNOSTIC CRITERIA OF DEPRESSION DSM4 Criteria A- Five symptoms from the mentioned list, but depressed mood or anhedonia are required. The symptoms must have been present all of the day, nearly every day for 2 weeks. 1.Depressed mood (sadness) 2.Anhedonia (lack of interest or pleasure in almost all activities) 3.loss of energy (fatigue) 4. Reduced self esteem or guilt 5.Reduced concentration or trouble making decisions 6. Recurrent thoughts of death or suicidal ideas 7. Psychomotor retardation or agitation (observed by others) 8. Sleep disorder (insomnia or hypersomnia) 9. Appetite loss, weight loss & appetite gain, weight gain
DIAGNOSTIC CRITERIA OF DEPRESSION Criteria B- The symptoms cause clinically significant distress or impairment in functioning (social, occupational or other areas) C- The symptoms are not due to Physical or organic factors or illness D-The symptoms are not better explained by bereavement (although this can be complicated by depression).
DIAGNOSTIC CRITERIA OF DEPRESSION A mnemonic for major depressive disorder is as follow: ==================================== SIG: EMCAPS 1) S = Sleep (hypersomnia) 2) I = Interest (lack of interest in life in general) 3) G = Guilt or hopelessness 4) E = Energy or fatigue 5) M =Mood (depressed, sad) 6) C =Concentration (lack of) 7) A =Appetite (increased or decreased, weight loss or gain) 8) P =Psychomotor (retardation or agitation) 9) S =Suicidal ideation ==================================== Major depressive disorder can be diagnosed based on presence of 5 out of 9 including no. (2 or 5).
SEVERITY OF DEPRESSION Each depressive episode could be graded according to the severity into mild, moderate or severe : ==================================== Mild to Moderate Depression • Threshold number (5) of symptoms with minimal functional impairment. • Marked symptoms and impairment of function. Severe depression All or nearly all symptoms and marked functional impairment in all areas of life ====================================
CLASSIFICATION OF DEPRESSION Primary Depression Unipolar • Major depressive disorder (single episode) • Recurrent depressive disorder (recurrent episodes) • Dysthyma Bipolar • Bipolar affective disorder • Cyclothyma Others • Seasonal affective disorder • Mixed anxiety and depressive disorder Secondary Depression
DIAFFERENTIAL D. OF DEPRESSION 1-Medical Mimics of Depression-Masquerades-2ry • Endocrine Disorders • Hypo/hyperthyroidism • Cushing's syndrome • Collagen V D (SLE/RA..) • Hematological D (Anemia) • Infectious D (Hepatitis;Influenza;HIV) • Neurological D • Dementia • Parkinsonism • CVS • Neoplastic D • Nutritional/Metabolic D • Hypokalemia/ hyponatremia • Uremia • Malnutrition particularly in elderly 2- Drug Induced Depression 3- Other Mental D
DIAFFERENTIAL D. OF DEPRESSION 2-Drug induced Depression • Cardiovascular agents • Beta B; CCB,Aldomet; Reserpine; Clonidine; Digitalis;Dyslipedemic D (Pravcastatin) • Respiratory Agents • Corticosteroids; Antituberculous D (INH) • GIT Agents • H2 antagonist • Neurological Agents • Carbamezapine • Phenytoin • PhenobarbitalParkinsonism • Gynecological Preparation • Contraceptives • Cancer Treatment • Psychotropic Agents • Benzodiazepines • Antipsychotic • Barbiturates
DIAFFERENTIAL D. OF DEPRESSION 3-Drug induced Depression Acute Psychotic Disorders Consider acute psychotic disorders if hallucinations (hearing voices, seeing visions) or delusions (strange or unusual beliefs) are present. Bipolar Disorder Consider bipolar disorder if history of manic episode (excitement, elevated mood, and rapid speech) is present. Alcohol Use Disorders Consider alcohol use disorders if there is a history of alcohol use. Dementia particularly among elderly
HOW DO YOU DIAGNOSE DEPRESSION ? Mental Assessment Consultation Interview and history taking Physical Examination Mental state Examination If we go through this process, it will lead to early and definite diagnosis of depression
CLINICAL PRESENTATION OF DEPRESSION WHO-ICD-10 • The patient may be presented initially with one or more physical symptoms (fatigue, pain). • Further inquiry will reveal depression or loss of interest. • Sometimes the depression presents as irritability. Presenting Complaints
CLINICAL PRESENTATION OF DEPRESSION WHO-ICD-10 Diagnostic Features • Low OR sad mood • Loss of interest OR pleasure • Associated symptoms are frequently present: • Disturbed sleep • Guilt or low self-worth • Fatigue or loss of energy • Poor concentration • Disturbed appetite • Suicidal thoughts or acts • Movements and speech may be slowed, but may also appear agitated. • Symptoms of anxiety or nervousness are frequently also present.
MANAGEMENT OF PATIENT WITH DEPRESSION Presenting the diagnosis Tell the patient that he/she has Depression Do not tell the patient that he/she has Depression How?? Exercise
Presenting the diagnosis A 45- year old- single woman came to see her family physician complaining of abdominal pain and nervous exhaustion. In the interview her physician noted that her affect was flat and that she spoke with long latencies. She was having trouble sleeping, frequent awaking after 4 hours, sleep with perspiration, heart palpitations, and obsessive worries about her job. She had assumed a new job 4 months earlier as manager of a hospital clinic that was converting to a new data management system. After the physician ascertained that the patient was not suicidal, She summarized the patient concerns and presented her diagnosis in the following dialogue:
Presenting the diagnosis Doctor: It is obvious that last few weeks have been like torture for you. It sounds like you carry a lot of responsibilities (including the working in the clinic that is depending on you). Let’s talk about what I think is going on and then I, d like to get your ideas about that. You have said that you are finding less energy during the day and that you awaken frequently at night, sometimes only getting a few hours, sleep. You tend to judge your self harshly, and lately you feel guilty that you are not accomplishing more. You have lost interest in things you used to enjoy, and lately all you can think about is your job. You are finding it harder to concentrate, and making simple decisions. Did I leave out anything?
Presenting the diagnosis Doctor: All these symptoms indicate to me that you are suffering from depression. This is an illness that affects our nervous system in way that robs us of our usual ability to enjoy the pleasure of life and to have confidence in our abilities. Your depressed mood is leading you to view yourself through a distorted lens that filters out all recognition of your competencies and abilities. [Pause to check patient’s response. After head nod from the patient, The doctor proceeds as follow] Any person is prone to that, fortunately, depression is very treatable illness and there are some very effective strategies you and I can work on together. This may be hard for you to believe right now, because of hopeless feeling that accompanies depression, but I’m quite confident that within a few weeks you will be feeling much better about yourself and about life.
Presenting the diagnosis Important Tips • Summarize the symptoms • May you add a couple of additional symptoms not mentioned by the patient to check their presence or absence. • Express the common existing of such illness to relieve the associated stigma. • May you use some diagrams to explain the illness • Emphasize on that depression is curable illness. • Discuss the available resources that may help in overcoming the stresses that precipitated the occurrence of depression.
MANAGEMENT OF PATIENT WITH DEPRESSION A) Essential Information for Patient and Family 1) Depression is common and effective treatments are available. 2) Depression is not weakness or laziness; patients are trying their hardest to cope. B) Specific Counseling to Patient and Family (1)Ask about risk of suicide. • Has the patient thought of death or dying? • Does the patient have a specific suicide plan? • Can the patient be sure not to act on suicidal ideas? • Close supervision by family or friends may be needed. How ?
SUICIDE RISK ASSESSMENT (SAD PERSONS INDEX) ========================================== Score > 7 means high suicide risk ========================================== • Sex • Age • Depression • Psychiatric history • Excessive drug use • Rationality loss • Separated • Organized plan • No support • Sickness • Male • <20 >45 years • Major Depression • Previous attempts • Substance abuser • Psychotic, s depression • Loss of spouse • Determined suicide plan • No back up ; isolated • Chronic illness 1 1 2 1 1 2 1 2 1 1
MANAGEMENT OF PATIENT WITH DEPRESSION B) Specific Counseling to Patient and Family (2) plan short-term activities, which give enjoyment or build confidence (3) Resist pessimism and self-criticism. • Do not act on pessimistic ideas (e.g. ending marriage, leaving job). • Do not concentrate on negative or guilty thoughts. (4)Identify current life problems or social stresses. • Focus on small, specific steps that patient might take towards reducing or better managing these problem. • Avoid major decisions or life change. How do you Help your Pt ?
MANAGEMENT OF PATIENT WITH DEPRESSION SPEAK Approach to help Pt to overcome Depression • Schedule • Pleasurable Activities • Exercise • Assertiveness (sharing other feeling) • Kind thoughts about your self (replace negative ones with positive)
MANAGEMENT OF PATIENT WITH DEPRESSION B) Specific Counseling to Patient and Family (5)If physical symptoms are present, discuss link between physical symptoms and mood (6) After improvement, discuss signs of relapse, plan with patient action to be taken if signs of relapse occur.
MANAGEMENT OF PATIENT WITH DEPRESSION C) Pharmacological treatment (1)Consider antidepressant drugs if sad mood or loss of interest is prominent for at least 2 weeks and 4 or more of associated symptoms are present: • In severe cases consider medication at the first visit. • If good response to one drug in the past uses that again. • If older or medically ill, use newer medication with fewer side effects. • If anxious or unable to sleep, use more sedating drug.
MANAGEMENT OF PATIENT WITH DEPRESSION C) Pharmacological treatment (2)Build up to effective dose (e.g. imipramine starting at 25 to 50 mg each night and Increasing to 100- 150 mg by I0 days) - lower doses if older or medically ill. (3) Explain how medications should be used: • Medication must be taken every day, • Improvement will build over 2-3 weeks. • Mild side effects may occur and usually fade in 7-10 days. • Check with the doctor before stopping medication. (4) Continue antidepressant at least 3 months after symptoms Improve.
MANAGEMENT OF PATIENT WITH DEPRESSION C) Pharmacological treatment Antidepressant Agents